www.cafamily.org.uk/know-your-rights/benefits-and-tax-credits/disability-living-allowance/
Benefit and tax credit rates,
calculator’s estimates are based on the information you supply to give you an idea of your potential entitlement UK
www.entitledto.co.uk/benefits-calculator/
Information on, benefits and grants and links to other useful sites. UK
patient.info/
Find out about Disability Living Allowance below UK
www.gov.uk/benefits-calculators
If your child was like me, they might be slow at talking? The link below might help you helping them to move forward.
http://teachmetotalk.com/2008/01/24/what-works-strategies-that-help-toddlers-learn-to-talk
NO Tube ( We can help your child learn to eat without a feeding tube)
http://www.notube.com
Look on the link below this to find out more from with in this website about EoE and EE
http://www.birth-defect.org/srapbook-page/
Eosinophilic Esophagitis (EE or EoE) is an emerging disease that is increasingly being recognized among pediatricians, internists, allergist, gastroenterologist (GI specialists), and other physicians. It is a condition that affects the esophagus and has been rising in incidence over the past decade.
EE Symptoms may include:
- Poor weight gain (failure to thrive)
- Refusal to eat
- Vomiting often occurring with meals
- Heartburn
- Difficulty swallowing (dysphagia)
- Pain or discomfort with swallowing (odynophagia)
- Food becoming lodged within the esophagus (food impaction)
A VERY INTERESTING READ
http://www.eosinophilicesophagitishome.org
Allergy Evaluation
A central component of the workup of eosinophilic esophagitis (EE or EoE) is the allergy evaluation. A number of studies have demonstrated that allergies when children with EE who have been placed on a diet of only a hypoallergenic elemental formula, in almost all cases they have rapid resolution of their symptoms, and normalization of their esophageal biopsies. This indicates that food allergies appear to be the main cause of this disease.
Although elemental formula diets are highly effective, they can be quite challenging to stay on, so the role of the allergist is to try to identify which food allergens may be triggering a patient’s disease so that they can be removed from the diet. There are 3 main ways in which food allergies can be detected in EE.
– Skin prick testing
– Blood allergy testing (eg. RAST)
– Atopy patch testing
http://www.eosinophilicesophagitishome.org/eosinophilic_esophagitis_diagnosis/eoe_diagnosis_allergy_testing/
BioGaia develops, markets and sells probiotic products with documented health benefits.
Constipation
The incidence of constipation among children varies between 7 and 30 percent depending on the country. A full 40 percent develop symptoms already during the first year of life and these often persist for a long time. Many children with constipation have continued problems as teens and adults.
http://www.biogaia.com
National information, advice and support service for carers in England
www.nhs.uk/carersdirecta
Website offering tips and advice in relation to kids’ behavior
www.kidsbehaviour.co.uk
Website offering advice regarding parenting after a separation or divorce
www.theparentconnection.org.uk
Employment law advice and solutions to individuals suffering from disadvantage or detrimental treatment in the workplace resulting from pregnancy or childbirth
www.babylaw.co.uk
Association for Children with life-threatening or terminal conditions and their families
www.togetherforshortlives.org.uk
At Sleeping Angels, we are all specially trained funeral facilitators who are compassionate and empathetic, patient and understanding.
We can’t change what’s happened but we can make the process of laying your baby to rest less stressful.
www.sleeping-angels.org.uk
Google CEO’s Condition Spotlights Vocal Cord Paralysis and Its Treatment
http://www.scientificamerican.com/article/google-ceo-page-vocal-fold-paralysis/
Parents of Down’s Syndrome voluntary support group
www.downs-syndrome.org.uk
LDA Learning are in partnership with associations such as ADDISS, Nansen, Afasic, Dyslexia Action and the Dyspraxia Foundation. They have resources and expertise for parents and teachers which cover the following conditions: Dyslexia, Dyscalculia, Dyspraxia, Autism, ADHD, Handwriting and Fine Motor Skills, Gross Motor Skills.
www.ldalearning.com
UK charity for people with autism (including Asperger syndrome) and their families. Information, support and pioneering services, and campaign for a better world for people with autism.
www.autism.org.uk/
Home-based therapy programme for children with developmental delay, brain injury due to birth trauma, accident, genetic conditions or chromosome abnormalities
www.brainwave.org.uk
The National Association for Special Educational Needs
www.nasen.org.uk
Independent School Search – Find and Compare Schools UK and Worldwide
www.isbi.com
National on-line resource and 24-hour access to a Health Visitor
www.healthvisitordirect.com
One for the kids. Go to the www.bbc.co.uk homepage for all BBC info (news, education, and entertainment.) If you’re in Hospital anywhere in the world
and you have the internet, try this out.
www.bbc.co.uk/cbbc
useful website
raisingchildren.net.au/articles/pip_homemade_baby_food.html
BOOKS
“The Marathon” by Kerry Sheeran (available on http://www.amazon.co.uk/The-Marathon-Kerry-Sheeran/dp/0991509706) is the true story of a mother and father forced to face something they never imagined could exist for their child. Follow their journey filled with extremes in marriage, parenting, and faith as their daughter faces EA/TEF head-on in Boston. A generous portion of the proceeds benefits Boston Children’s Hospital- so that families like ours can benefit from the ground-breaking research & care they provide.
www.kerrysheeran.com
New Book from The USA to help explain to Children and Parents being born unable to swallow, shipped out across the world
http://www.eatefbooks.com/
FREE MAG’S
Every issue of ABC Magazine is packed full of local information and practical parenting advice to help you find what you need and where to buy it, ideas on what to do and where to go, where to find this and that – all child related and child friendly! Loads of articles, great competitions, true-life stories, health updates, all sorts of parenting advice, facts and figures, ideas to fill your days and masses of useful practical parenting tips to help put you on the right road for early parenthood.
http://www.abcmag.co.uk/
~
Non-Operative Correction for Long-Gap Esophageal Atresia
Boston Children’s Hospital
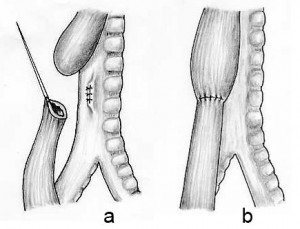
About 1000 infants a year in the states are born with their esophagus disconnected, which is called Esophageal Atresia (EA). The standard operation for esophageal atresia is Foker process, which requires several thoracotomies for placing traction sutures on esophageal ends, followed by primary anastomosis. There have been attempts to develop non-operative method for correcting esophageal atresia, especially by using magnetic force. Hendren et al. explored electromagnetic bougienage method to correct long gap esophageal atresia. Zaritzky et al. presented a method of magnetic compression anastomosis, which took advantage of large attracting force between two rare-earth permanent magnets.
In our research, a non-operative correction method for long-gap esophageal atresia is proposed. A magnetic-tipped catheter was designed for bougienage and compression anastomosis. The magnetic tip comprises syringe mechanism with an outer barrel, which functions as a fluidic stand-off. The pressure of the fluid could be measured externally so as to estimate the tip force. The catheter moves back and forth by friction drive (long stroke), and the syringe mechanism at the tip also generates more displacement (short stroke).
A pair of the magnetic catheter is put into proximal and distal esophageal pouches respectively. They apply cycling stretching force on esophagus to stimulate it to grow. Once the esophagus grows in sufficient amount, the fluid in the magnetic syringe could be drawn off for magnetic compression anastomosis; the large force between two magnets squeezes the esophageal tissue, necrosis and regeneration of the sandwiched tissue leading to the compression anastomosis.
A HYDRAULICALLY CONTROLLED NONOPERATIVE MAGNETIC TREATMENT FOR LONG-GAP ESOPHAGEAL ATRESIA, very interesting
http://web.mit.edu/2.75/projects/DMD2011-5231.pdf
Back Pain?
Learn about back pain and how to help yourself.
http://healthofback.com/